|
EVALUATION
OF THE CHEST X-RAY |
|||||||||||||||
|
Technical
quality |
|||||||||||||||
 DENSITY DENSITYVertebral bodies must be VISIBLE through the cardiac shadow |
|||||||||||||||
 POSITION
of the SCAPULAE POSITION
of the SCAPULAEThey should project outside the lung fields wrong---> correct: |
|||||||||||||||
|
ROTATION Medial ends of the claviculae should be EQUIDISTANT from the spinous process |
|||||||||||||||
|
INSPIRATION Anterior segment of the 6th rib Posterior segment of the 9th rib ABOVE the DIAPHRAGM |
|||||||||||||||
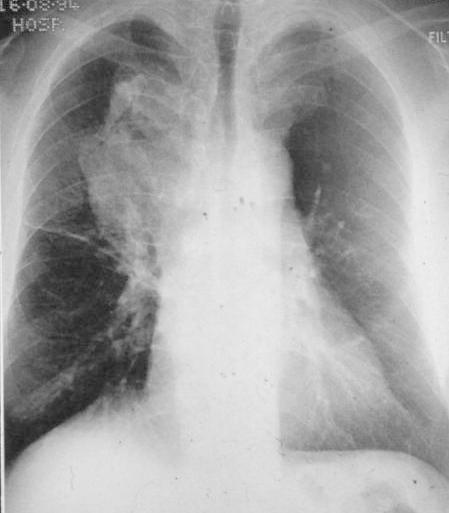
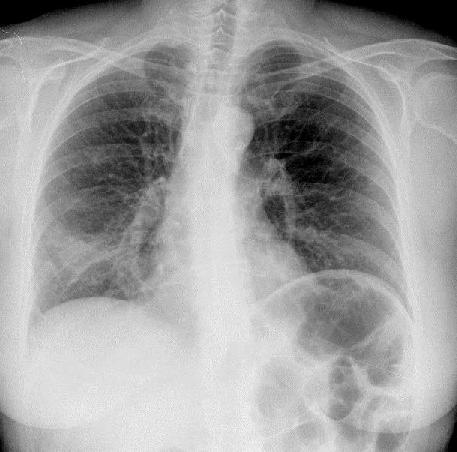
 INSPIRATION INSPIRATIONPoor Inspiration (picture to the right -->): * False enlarged heart * Difficult evaluation of the lungs Same patient on inspiration (below):  |
|||||||||||||||
|
THE
NORMAL CHEST X-RAY 1. Heart 2. Hila 3. Mediastinum 4. Lungs 5. Diaphragm 6. Chest wall 7. Pleura + sinuses |
|||||||||||||||
 The
Heart The
Heart1. Always look at both films 2. Right border: Edge of (r) Atrium 3. Left border: (l) Ventricle + Atrium |
|||||||||||||||
 The
Heart - lateral film The
Heart - lateral film4. Posterior border: left Ventricle 5. Anterior border: right Ventricle |
|||||||||||||||
 The
Hila The
Hila1. Made of: * Pulmonary Art. + Veins * The Bronchi 2. Left Hilus higher (max 1-2,5 cm) 3. Identical: size, shape, density |
|||||||||||||||
 The
Mediastinum The
Mediastinum1. Look at both films 2. The edges should be clear 3. Right sup.border: * Innominate vessels + Sup. vena cava 4. The (r) paratracheal line (2-3 mm) 5. Left sup. border: * Subclav.art. + Arcus aorticus (2-3 cm) |
|||||||||||||||
 The
LUNGS The
LUNGS1. Equal density 2. Symmetrical 3. Look for the Minor Fissure (from the right hilus to 6th rib) 4. Look for the Major fissure (lateral) (from T4-5 to the diaphragm) |
|||||||||||||||
|
The
diaphragm 1. Both Hemi. clearly VISIBLE 2. Both have CONVEX shape 3. The right is HIGHER (1-3 cm) |
|||||||||||||||
 The
Lateral Films The
Lateral Films1. Lung Fields in front and behind the heart = Same Density 2. Density over the heart = density over upper thoracic spine |
|||||||||||||||
| The
Lateral Films 3. Check the position of FISSURES 4. The Hila (density, size, etc) 5. Vertebral bodies |
|||||||||||||||
|
Additional
Views 1. Expiration views 2. Decutitus (lateral) 3. Rib views |
|||||||||||||||
|
The
Abnormal Chest X-Ray 1. Heart failure 2. Enlarged Hila 3. Enlarged Mediastinum 4. Lung disease: (infection, emboli, pneumothorax, emphysema, "Coin lesion") |
|||||||||||||||
| 1.
Heart failure Radiological Signs: a) Enlarged heart shadow C.T. index > 50 % b) Vascular redistribution |
|||||||||||||||
| 1.
Heart failure c) Kerley lines "B" d) Pulmonary Edema: e) Pleural fluid |
|||||||||||||||
 The
Enlarged Hila The
Enlarged HilaCauses: 1. Adenopathies (neoplasia, infection) 2. Primary Tumor 3. Vascular 4. Sarcoidosis |
|||||||||||||||
|
The
Enlarged Hila Diagnostic approach: Chest X-Ray (2 planes) |
|||||||||||||||
|
The
Enlarged Mediastinum 1. Always EXCLUDE rotation 2. Causes: Superior / Anterior * Thymoid * Thymus * Innominate artery * Lymphoma |
|||||||||||||||
 The
Enlarged Mediastinum The
Enlarged Mediastinum3. Causes: Middle / Inferior * Lymphoma * Aortic aneurysm * Dilated eosophagus |
|||||||||||||||
|
The
Lung diseases 1. INFECTIONS a) TBC b) Pneumonia |
|||||||||||||||
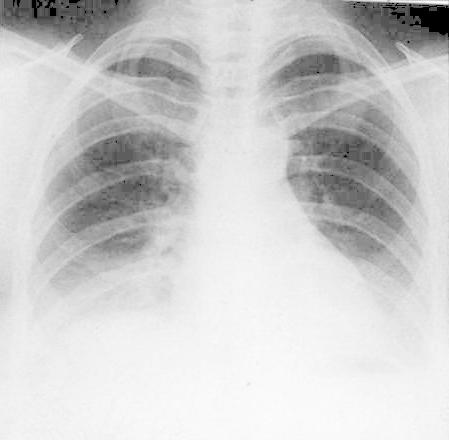
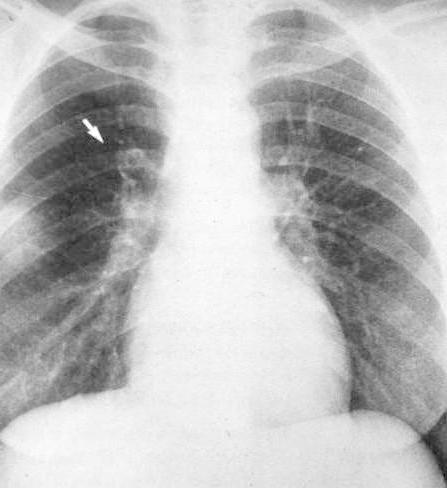
 Tuberculosis TuberculosisTBC signs: 1. Reticulo - Nodular 2. Apical + Parahilar 3. Uni- og Bilateral |
|||||||||||||||
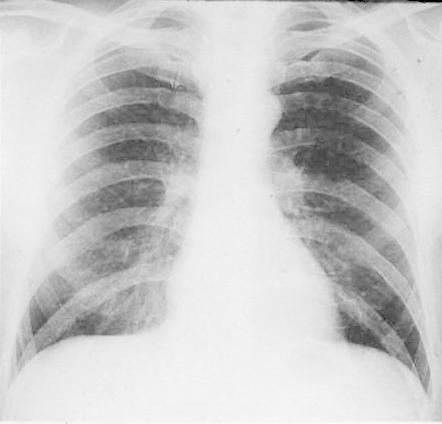
 Pneumonia PneumoniaCharacteristics: 1. Infiltrate + "Air bronchogram" 2. Diffuse, Homogeneous 3. Location: * Uni- og Bilateral * Segmental or Lobar |
|||||||||||||||
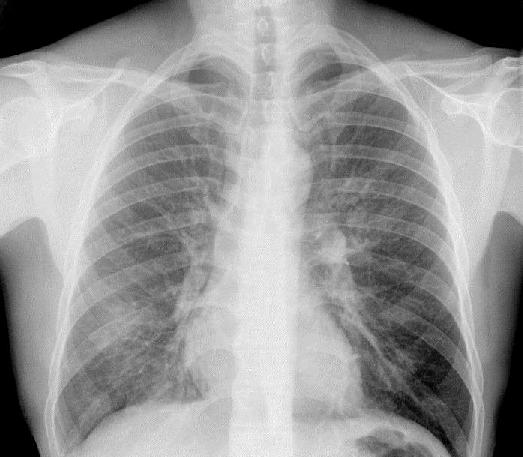
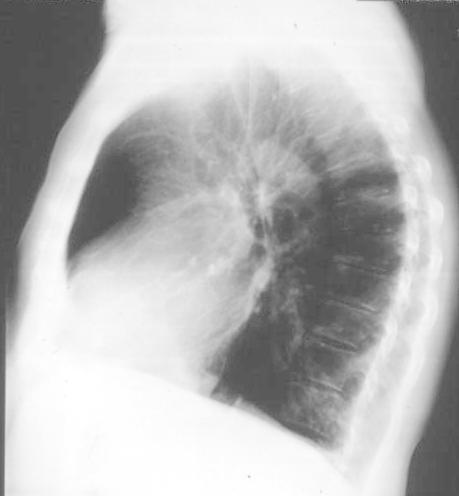
 Pneumonia PneumoniaThe "Silhouette" Sign = Indistinct Heart Border Location: Middle lobe or Lingula Example: Pneumonic infiltrate in upper segment of middle lobe (r) visible as indistinct heart border in frontal projection and clearly visible in lateral projection  |
|||||||||||||||
Fibrosis
Vs Infiltrate
|
|||||||||||||||
|
|||||||||||||||
 Pulmonary
emboli Pulmonary
emboliFrequent Signs: 1. Darker area of Reduced Perfusion (Westermark's sign) 2. "Cut off" sign 3. Focal Consolidation (infarction) |
|||||||||||||||
 Pneumothorax PneumothoraxX-Ray signs: 1. Pleural line 2. No parenchym behind the line 3. Displacement of mediastinum |
|||||||||||||||
|
The
"Coin Lesion" Definition: "A well circumsc. shadow in the lungs" Causes: * Tumor (benign or malignant) * Infection (eg. abscess, TBC) * Cyst (Hydatid), Rheuma, nodule |
|||||||||||||||
 The
"Coin Lesion" The
"Coin Lesion"# Always look at old films Signs of Malignency: * Irregular borders * Prominence of additional lesions * Parahilar mass + bone lesion(s) |
|||||||||||||||
|
The
Coin Lesion # If Malignant signs present or if (?) CT Scan |
|||||||||||||||
|
CONCLUSION 1. "Good" Technique 2. "Good" Look at both films 3. "Good" LUCK |
|||||||||||||||
| Author:
Claude Pierre-Jerome Edited by: Arne Westgaard, 14.12.2000. Updated 31.03.2003. |

|
|